Leiden Sie an Luftnot bei körperlicher Belastung oder gar an Atemnot beim Sprechen und in Ruhe? Kein Arzt findet eine Ursache und kann Ihnen helfen? Hier erfahren Sie mehr zur Bedeutung eine verringerten Atemmuskelkraft und Apnoetoleranz und wie Sie Ihre Leistungsfähigkeit verbessern können!

Eine schwache Atemmuskulatur und eine verringerte Apnoetoleranz werden als Ursache der Luftnot von Ärzten und Physiotherapeuten fast immer unterschätzt.
Gerade nach einer Erkrankung, wie zum Beispiel einer Corona-Infektion bleibt häufig eine Einschränkung der körperlichen Leistungsfähigkeit bestehen. Das Hauptsymptom ist eine Belastungsluftnot. Da die Beschwerden nicht besser werden, besuchen Sie den Hausarzt und verschiedene Fachärzte. Häufig wird die Ursache nicht gefunden und Sie bleiben sich selbst überlassen.
In der Cardiopraxis® machen wir tagtäglich die Erfahrung, dass eine Einschränkung der Atemmuskelkraft und eine verringerte Apnoetoleranz sehr häufig eine Ursache für Luftnot sind und können so gezielt helfen.
Luftnot und Atemnot – Ursache häufig nicht gefunden
Der Begriff Dyspnoe (altgriechisch: „δυσ“ „dys“ „schwierig“ und „πνοή“ „pnoe“ „Atmung“) wird im Deutschen meistens gleichgesetzt mit Luftnot, Atemnot, Lufthunger und Kurzatmigkeit. Vereinfacht betrachtet bedeutet Luftnot ein Missverhältnis zwischen dem Bedarf Ihres Körpers an Gasaustausch, das heißt einer Aufnahme von Sauerstoff und einer Abgabe von Kohlendioxid und dem Angebot an Luft über die Lunge, das heißt. Kurzum bei Luftnot der Bedarf größer ist als das Angebot.
Typischerweise kennen wir Luftnot, wenn wir uns körperlich belasten und entsprechend wird der Schweregrad der Luftnot auch eingeteilt in Luftnot bei:
- schwerer körperlicher Belastung
- mittelschwerer körperlicher Belastung
- leichter körperlicher Belastung
- in körperlicher Ruhe und beim Sprechen
Die Luftnot bei körperlicher Belastung kann auch abgegrenzt werden von der Luftnot in körperlicher Ruhe und bei Sprechen, welche wir dann auch Atemnot bezeichnen können. Atemnot ist gekennzeichnet durch eine flache und schnelle Atmung, tritt in Ruhe vor allen Dingen nach Mahlzeiten auf und ist meistens mit Problemen beim Sprechen verbunden.
Im gesamten ambulanten medizinischen Versorgungsbereich leiden circa 25% der Patienten an Luftnot aller Schweregrade. In einzelnen Fachrichtungen, wie zum Beispiel der Kardiologie sind es bis zu 50%. Trotz umfangreicher hausärztlicher und fachärztlicher Abklärung wird bei 30-50% der betroffenen Menschen eine Ursache nicht gefunden und sie bleiben sich selbst überlassen.
Hausärzte, Internisten, Pneumologen, Kardiologen, Physiotherapeuten – Atemmuskelkraft wird nicht gemessen
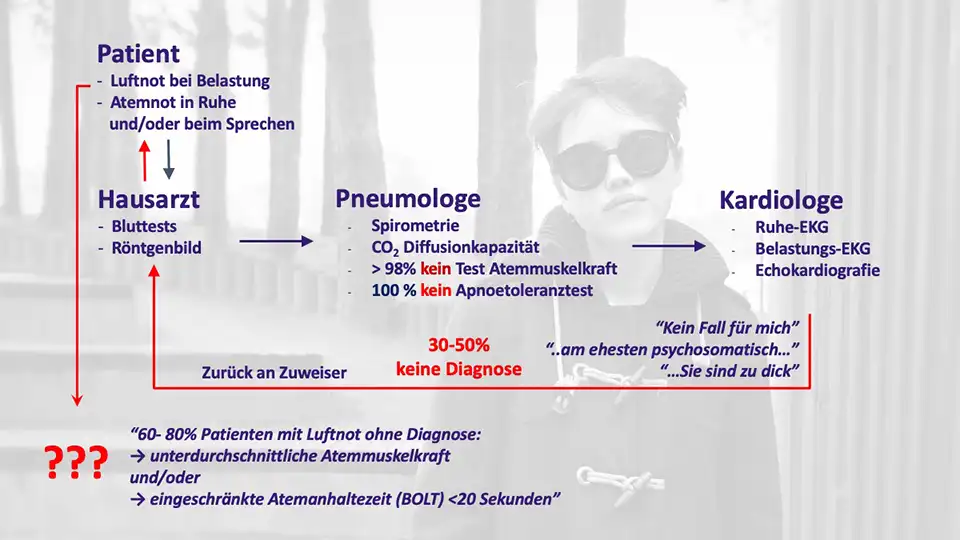
Menschen mit Luftnot haben häufig eine reine monatelange Irrfahrt durch das medizinische System hinter sich. Wenn Sie an Luftnot leiden, dann gehen Sie in der Regel als erstes hilfesuchend zu Ihrem Hausarzt.
Hausarzt. Sie schildern Ihrem Hausarzt zunächst eingehend Ihre Symptome und er untersucht Sie dann gründlich körperlich. Er misst den Blutdruck s sowie die Herzfrequenz und führt Laboruntersuchungen durch, um zum Beispiel eine Blutarmut oder eine Infektionserkrankung auszuschließen.
Wenn der Hausarzt keine Ursache der Luftnot findet, dann gibt er Ihnen in der Regel eine Überweisung zum Lungenfacharzt und zum Kardiologen, meistens in dieser Reihenfolge.
Lungenfacharzt. Sie schildern dem Lungenfacharzt zunächst eingehend Ihre Symptome und er untersucht Sie dann gründlich körperlich. Er führt die übliche Messung zur Bestimmung der Weite der Atemwege und des Lungenvolumens, die Spirometrie durch. Eventuell werden CO-Transfer (Leitfähigkeit der Lunge für Blutgase), Blutgasanalyse und ein Röntgenbild der Lunge durchgeführt. Wenn der Lungenfacharzt nichts findet, dann verweist er Sie an den Kardiologen und gibt Ihnen vielleicht noch ein Asthma-Spray mit.
Kardiologe. Sie schildern dem Kardiologen zunächst eingehend Ihre Symptome und er untersucht Sie dann gründlich körperlich. Er führt die üblichen Messungen EKG, Belastungs-EKG und Herzultraschall durch. Wenn der Kardiologe nichts gefunden hat, dann schickt er Sie zurück zu Ihrem Hausarzt.
Physiotherapeuten. In seltenen Fällen werden Sie zum Atemtraining zur Atemtherapie an einen Physiotherapeuten überwiesen. Dort werde fast immer nur Verspannungen gelöst, um das Lungenvolumen zu vergrößern und die Atmung zu erleichtern. Ein gezieltes Training der Atemmuskelkraft oder gar ein Apnoetraining erfolgt nicht.
Einschränkung der Atemmuskelkraft häufig unerkannter Grund für Luftnot
Wie bereits angeführt, gehen 30-50% der Menschen mit Luftnot diesen zum Teil sehr langwierigen Weg, ohne dass eine fassbare Ursache für die Luftnot gefunden worden ist. Nicht selten müssen Sie sich Kommentare anhören, wie zum Beispiel: „sie sind zu dick“, „sie müssen sich mehr bewegen“, „sie sind ja auch schon älter“, „möglicherweise ist das auch Long-COVID“, „vielleicht ist das auch psychosomatisch“ und, und, und. Am Ende stehen Sie ziemlich allein da mit Ihrer Luftnot: nicht erkannt und nicht behandelt.
Was gemäß eigenen Erfahrungen bei dieser Kaskade an medizinischen Maßnahmen in >99% der Fälle nicht geschieht ist eine Messung beziehungsweise richtige Bewertung der Atemmuskelkraft und der Apnoetoleranz. In der Cardiopraxis weisen nach Ausschluss aller anderen Ursachen 60-80% der symptomatischen Patienten eine unterdurchschnittlich Atemmuskelkraft und/oder eine verkürzte Atemanhaltezeit bis zum ersten Atemantrieb nach entspannter Ausatmung von <20 Sekunden auf.
Ursache der Einschränkung der Atemmuskelkraft ist in fast allen Fällen eine falsche Atemtechnik mit einer flachen Mund-Brustatmung. Die Mund-Brustatmung führt über eine zu geringe Beanspruchung des Zwerchfells zu einer muskulären Schwächung dieses Hauptatemmuskels und ist schlichtweg eine schlechte Angewohnheit.
Atemmuskelkraft – messen, bewerten, trainieren
Die Messung der Atemmuskelkraft erfolgt sehr selten, obwohl medizinisch zugelassene sogenannte „stand-alone“ Geräte ab 1.500 Euro auf dem Markt erhältlich sind, zum Beispiel der MicroRPM. Diese Geräte könnten sowohl von Hausärzten, Internisten, Lungenfachärzten, Kardiologen, aber auch von Anästhesisten und Chirurgen zur Vorbereitung von Operationen leicht genutzt werden. Auch für Physiotherapeuten macht eine solche Messung Sinn, um die Leistungsfähigkeit der betreuten Menschen gezielt zu verbessern.
Zum Teil ist die Messung der Atemmuskelkraft auch in größere Geräte integriert, die von Lungenfachärzten zur Bestimmung anderer Lungenparameter genutzt werden.
Neben der Tatsache, dass die Messung der Atemmuskelkraft fast nicht eingesetzt und die gesundheitliche Störung nicht erkannt wird, ist die Unkenntnis von vergleichenden Referenzwerten ein Problem. Allerdings gibt es wissenschaftlich etablierte Messwerte.
Mittelwert Inspirationskraft bezogen auf Alter und Geschlecht
- Männer = 120 – (0,41 x Alter) cmH2O
- Frauen = 108 – (0,61 x Alter) cmH2O
Mittelwert Expirationskraft bezogen auf Alter und Geschlecht <100%
- Männer = 174 – (0,83 x Alter) cmH2O
- Frauen = 131 – (0,68 x Alter) cmH2O
Werte unterhalb des Mittelwertes sind als therapie- beziehungsweise bedürftig einzustufen. Problematisch bei diesen Mittelwerten ist, dass Körpergröße und Körpergewicht nicht in die Bewertung einbezogen werden, obwohl sie eine erhebliche Relevanz haben. Gerade überdurchschnittlich große und schwere Menschen müssen eher behandelt werden. Hier müssen in der Zukunft noch Formeln wissenschaftlich entwickelt werden, die den Aspekt von Körperlänge und Körpermasse mit einbeziehen.
Atemmuskeltraining wird sehr, sehr selten verordnet, obwohl es hierfür gymnastische Übungen gibt und Trainingsgeräte im Handel erhältlich sind. Trainingsgeräte werden fast ausschließlich bei der post-operativen Rehabilitation genutzt. Wenn eine Atemtherapie verordnet wird, dann beschränken sich Physiotherapeuten fast ausschließlich auf Lösung von Verspannungen und Erweiterung des Lungenvolumens.
Verringerte Apnoetoleranz – messen, bewerten, trainieren
Die Apnoetoleranz ist mit Atemanhalte-Test nach entspannter Ausatmung leicht selbst messbar. Bei Werten < 20 Sekunden ist ein Training erforderlich. Das Apnoetraining kann durch einfache Atemmuster mit in Ruhe oder beim Gehen im Alltag ganz beiläufig geübt werden und führt rasch zu Erfolgen.
Praktisches Vorgehen für Menschen mit Luftnot und Verdacht auf Atemmuskelschwäche und/oder einschränkte Apnoetoleranz
Wenn Sie den als Betroffener den Verdacht haben, dass bei Ihnen eine Atemmuskelschwäche oder eine eingeschränkte Apnoetoleranz vorliegt, dann stehen Sie zunächst einmal ziemlich allein da, weil Ihnen Ärzte und Physiotherapeuten in den meisten Fällen nicht weiterhelfen und sich damit meistens selbst helfen müssen.
Grundlage jeder Selbsthilfe bei Luftnot ist, dass, Lungenerkrankung und Herz-Kreislauferkrankung einschließlich eines schlecht eingestellten Bluthochdrucks als Ursache von Luftnot medizinisch ausgeschlossen werden. An einem Besuch beim Pneumologen und eines Kardiologen kommen Sie also nicht vorbei.
Optimales Vorgehen bei Atemmuskelschwäche und eingeschränkter Apnoetoleranz
Optimal ist, wenn Atemmuskelschwäche beziehungsweise eine eingeschränkte Apnoetoleranz durch Messwerte bewiesen ist.
Aufbauend auf den Messwerten kann dann ein Atemmuskeltraining und/oder Apnoetraining unter medizinischer Kontrolle (Arzt, Physiotherapeut) erfolgen. Das hilft bei der Fehlervermeidung, gerade bei Menschen mit langjähriger Fehlatmung; hier benötigen gerade ältere Menschen viel Zuwendung und Anleitung.
Die Therapiekontrolle erfolgt dann über eine wiederholte Bestimmung der Messwerte und eine gezielte Anpassung der Therapie.
Suboptimales Vorgehen – Selbsthilfe bei Training von Atemmuskelkraft und Apnoetoleranz
Wenn Ihnen aus medizinischer Sicht niemand helfen kann (oder will), relevante Lungen- und Herz-Kreislauferkrankungen medizinisch ausgeschlossen, dann können Sie daran gehen sich selbst zu helfen.
Als erstes sollten Sie eine reine Nasen-Zwerchfellatmung in den Bauch, das heißt Einatmung und Ausatmung nur durch die Nase erlernen und in allen Lebenssituationen durchführen. Hinzu kommt ein aktives Gehen mit mehr Körperspannung im Alltag.
Eine Einschränkung der Apnoetoleranz können Sie mit dem Atemanhalte-Test nach entspannter Ausatmung selbst messen. Mit einfachen Übungen können Sie diese die Apnoetoleranz steigern.
Das Training der Atemmuskulatur können Sie mit einfachen Übungen beginnen. Prinzip ist dabei eine Nutzung von Führungswiderständen, zum Beispiel im Sitzen mit einem Kissen oder einem Medizinball und bei der Gymnastik mit Umkehrpositionen, zum Beispiel der Schulterbrücke.
Gut geeignet zur Steigerung der Atemmuskelkraft sind apparative Atemmuskeltrainer. Hier gibt es sehr einfache und preiswerte Geräte, die Onlinehandel oder im Sanitätshaus erhältlich sind.
Allerdings zeigt unsere Erfahrung in der Cardiopraxis, dass zur vollen Ausschöpfung Ihres individuellen Potentials die wiederholte messtechnische Bestimmung der Atemmuskelkraft sehr hilfreich ist. Der AiroFit Pro bietet ihnen hier neben App-gesteuerten Programm zur Steigerung von Apnoetoleranz und Atemmuskelkraft die die entsprechenden messtechnischen Möglichkeiten zur Bestimmung der maximalen Einatmungskraft und Ausatmungskraft. Diese Messwerte sind mit den Ergebnissen der medizinisch zugelassenen Geräte vergleichbar.
Achten Sie beim Atemmuskeltraining auch auf Nebenwirkung, ein „over training“ sollten Sie vermeiden. Die Trainingseinheiten sollten so gestaltet sein, dass Sie zwar leicht angestrengt sind, aber sich nicht erschöpfen.
Atemmuskeltraining kann auch Herz-Kreislauferkrankungen und Lungenerkrankungen, wie zum Beispiel Bluthochdruck, niedrigem Blutdruck, Benommenheit, Herzschwäche und chronisch-obstruktiver Atemwegserkrankung sehr erfolgreich zur Leistungssteigerung durchgeführt werden. Allerdings sollte das unter ärztliche Kontrolle erfolgen.